Local Excision (Wide local excision, lumpectomy)
This procedure is performed in a similar fashion to benign breast biopsy, with the main difference being that a larger margin of tissue is removed with the tumour to ensure adequate clearance. The incision may be placed over or close to the tumour in a skin crease, or ideally in a cosmetic position around the areola Commonly the incision would be 4-5cm in length but is individualised. Once removed, the breast tissue would be approximated to minimise any cosmetic deformity. The skin is closed with dissolvable sutures. Results are usually available on the pathology within two to three days so that further management can be planned. Despite the best of intentions, sometimes microscopic disease is not apparent at operation and clearance margins on the edge of the excision may be inadequate, requiring re-operation; either re-excision of margins or mastectomy. For invasive cancer, lumpectomy is usually combined with a sentinel lymph node biopsy or axillary clearance.
Mastectomy
Mastectomy for breast cancer involves excision of the breast tissue down to the underlying muscle (pectoral muscle). There are several types of mastectomy as described below. These include the traditional simple mastectomy, which is still performed but often when reconstruction is offered it is replaced with skin sparing or nipple sparing mastectomy.

Simple Mastectomy
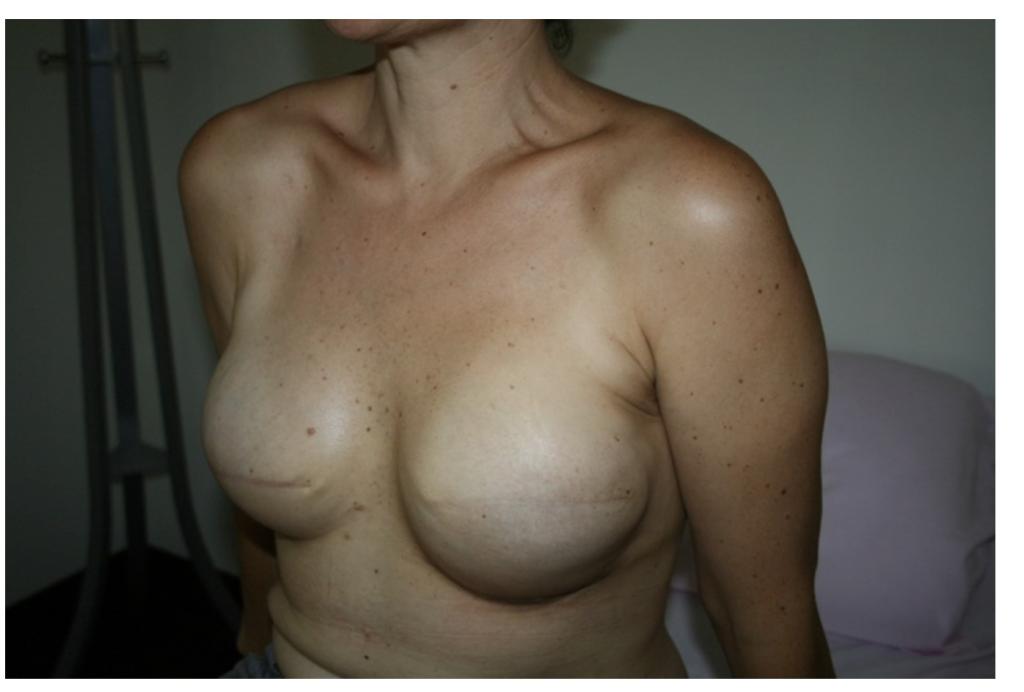
Simple mastectomy
Involves complete removal of the nipple and areola as well as the surrounding skin with the underlying breast tissue down to the pectoral muscle. This will results in a flat chest wall so that an external prosthesis in a bra can be used if desired. As seen in the adjacent photo, the scar extends from the inner aspect of the breast into the auxillar (under the arm) to a variable extent. Sensation can be temporarily or permanently lost or reduced on the chest wall.
Skin Sparing Mastectomy
This involves removal of all the breast tissue and nipple areolar complex but preserves more surrounding skin so that reconstruction can be performed. It is often utilised in larger breasted patients with the advantage of making the reconstructed breast smaller. Again, dissolvable sutures and drains are utilised.
Skin sparing mastectomy with implant reconstruction

Nipple Sparing mastectomy and implant reconstruction with scars hidden in the inframammary folds (bottom of the breast)
Nipple Sparing Mastectomy
This involves preservation of all of the breast skin including the nipple and areola and allows breast reconstruction to be performed with improved cosmetic results. It may not be possible to preserve the nipple if the breast is very large or if involved with cancer. There is also a 5-10 % risk of loosing the nipple due to poor blood flow (necrosis). When done well, with appropriate removal of tissue behind the nipple, there is no evidence of any increased risk of cancer recurrence with nipple sparing. Scars can be hidden along the lower folds of the breast to improve cosmesis however sometimes may need to be placed around the nipple or elsewhere. It should be noted that breast skin and nipple sensation will be lost or significantly reduced.